CASE REPORT
https://doi.org/10.47811/bhj.206
Purple urine bag syndrome in a young man with paraplegia in Bhutan: a case report
Karma Tenzin1 , Kinley Zangmo2 , Tshetrim Zangmo1
1Phuntsholing General Hospital, Chhukha, Bhutan
2Gedu Hospital, Chhukha, Bhutan
Corresponding author:
Karma Tenzin
ktenzin00@gmail.com
ABSTRACT
Purple urine bag syndrome is an uncommon clinical phenomenon characterized by purple discolouration of the urinary catheter bag. It typically affects elderly, immobilized, and co-morbid patients on long-term urinary catheters. The purple discolouration is due to the production and mixing of pigments indirubin and indigo in the presence of bacteria in the urine. While often benign and asymptomatic, it can signal an underlying urinary tract infection and has been associated with severe complications. We present the case of a 20-year-old man with paraplegia on a permanent suprapubic catheter, who developed purple urine bag syndrome accompanied by systemic signs of infection. His urine culture identified Staphylococcus aureus, an organism not frequently associated with the condition. The patient achieved full recovery with no recurrence during follow-up. Healthcare providers need to be aware of this condition to ensure timely recognition, assessment, and appropriate management.
Keywords: Purple urine bag syndrome; Staphylococcus aureus; Urinary catheter; Urinary tract infection.
INTRODUCTION
Purple Urine Bag Syndrome (PUBS) is an intriguing and uncommon clinical occurrence where the urinary catheter bag and tubing acquire a purple discolouration. The urine itself is not always noted to be purple1. It results from a series of reactions starting with dietary tryptophan and enzymes produced by bacteria in the urine2. PUBS itself is benign but can be a manifestation of an underlying urinary tract infection3. It predominantly affects comorbid elderly patients with long-term urinary catheters who are immobilized, institutionalized, and chronically constipated1,4.
It can cause anxiety in patients and caregivers1,3. The diagnosis can be missed by unsuspecting healthcare providers5. We present the first reported case of PUBS in Bhutan to increase awareness among our healthcare providers. The patient presented to Phuntsholing Hospital but, as per his preference, was admitted to Gedu Hospital for treatment in December 2025.
PATIENT INFORMATION
A 20-year-old male with paraplegia presented with a one-day history of fever associated with chills, rigor, vomiting, malaise, and poor oral intake. His caregivers were concerned about the sudden purplish discolouration of his urine bag, noted on the morning of presentation. The patient had not used any medications, including traditional remedies, prior to presentation. Despite reporting recent bowel movements upon presentation, the patient had a history of intermittent constipation.
His paraparesis dates back to 2021 when he was diagnosed with an intramedullary spinal tumour extending from T8 to T12. Histopathological examination identified ganglioglioma, pilocytic astrocytoma, and diffuse midline glioma as differential diagnoses, with further immunohistochemistry required for confirmation. However, COVID-19-related travel restrictions prevented his referral abroad for further management, and he was subsequently lost to specialist follow-up.
Since 2021, the patient has been wheelchair-dependent and on a suprapubic urinary catheter. The catheter is replaced every four weeks, with the most recent change being one week prior to presentation.
CLINICAL FINDINGS
On examination, he appeared ill but was conscious and oriented. His temperature was 37.4 degrees Celsius; pulse rate was 128 beats per minute; blood pressure was 141/90 mmHg. The abdominal examination revealed no tenderness. Respiratory and cardiovascular examinations were unremarkable.Neurological examination of the lower limbs revealed muscle wasting, joint contractures, and paraplegia with sensory level at T12. Both the urine bag and the drainage tube showed purple discolouration (Figure 1). However, the urine itself was dark red.
DIAGNOSTIC ASSESSMENT
Laboratory investigations revealed neutrophilic leukocytosis with an elevated C-reactive protein and mild thrombocytopenia (Table 1). Urine microscopy showed significant pyuria and haematuria, while renal function was preserved. Screening for dengue, malaria and scrub typhus was negative.
Our working diagnosis was PUBS due to complicated urinary tract infection.
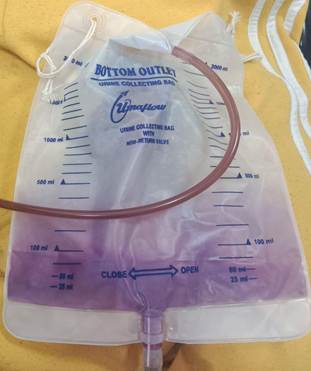
Figure 1. Purple discolouration of patient's urinary bag and drainage tube.
THERAPEUTIC INTERVENTION
The catheter was immediately replaced under aseptic conditions. Urine samples for microscopy and culture were obtained during the procedure. Following admission, he was managed with intravenous ceftriaxone (1 g every 12 hours), intravenous fluids, intravenous metoclopramide, and oral paracetamol.
During hospitalization, the patient remained afebrile. His appetite and general clinical condition improved, with no recurrence of the purple discolouration in the urinary collection system.
On the third day of admission, his urine culture revealed significant (>105 CFU/mL) growth of Staphylococcus aureus. The isolate was sensitive to cloxacillin, cefoxitin, nitrofurantoin, norfloxacin, and co-trimoxazole. Consequently, ceftriaxone was discontinued, and intravenous cloxacillin (1 g every 6 hours) was initiated.
Follow-up laboratory investigations on the fourth day of admission showed marked improvement in the leucocyte count and C-reactive protein and platelet counts (Table 1). After receiving intravenous cloxacillin for 48 hours, he was discharged on a 10-day course of oral cloxacillin (500 mg every 6 hours).
Table 1. Summary of laboratory investigation findings of a 20-year-old male with paraplegia, treated for purple urine bag syndrome due to complicated urinary tract infection
|
Test parameter |
Day 1 |
Day 4 |
Reference Range |
|
WBC |
15.38 |
6.30 |
3.61-9.56x103/μL |
|
Neutrophil |
13.89 |
4.04 |
1.96-6.50x103/μL |
|
Haemoglobin |
14.80 |
13.20 |
14.00-18.40 g/dL |
|
Platelet |
137 |
313 |
138-450x103/μL |
|
CRP |
146.21 |
34.91 |
0.00-6.00 mg/L |
|
Urea |
44.75 |
17.74 |
10-50 mg/dL |
|
Creatinine |
0.96 |
0.70 |
0.9-1.3 mg/dL |
|
Urine culture |
Staphylococcus aureus |
||
CRP:c-reactive protein; WBC:white blood cell
FOLLOW - UP AND OUTCOMES
The patient was reviewed after completion of his oral antibiotic course. He remained asymptomatic, and the purple discolouration of the urine bag had not recurred. A repeat urine culture yielded mixed microbial growth, suggestive of contamination during sample collection. The patient and his caregivers were counselled regarding the nature of his spinal tumour, and were advised for follow-up assessment with a spine surgeon.
DISCUSSION
PUBS was first reported in 1978 by Barlow and Dickson6. The purple discolouration was studied to be from mixing of two pigments: indirubin (red) and indigo (blue). Dietary tryptophan is metabolized into indole by intestinal bacteria and transported to the liver. There, indole undergoes hepatic conjugation and is excreted into the urine as indoxyl sulphate. Subsequently, bacteria with phosphatase and sulphatase enzymes catalyse the breakdown of indoxyl sulphate in urine to produce indirubin and indigo2. The most commonly identified bacteria in patients with PUBS are Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis and Pseudomonas aeruginosa1,4,5.
A 2017 systematic review with meta-analysis of 281 patients with PUBS, reported a prevalence of 11.7% among chronically catheterized patients4. While PUBS predominantly affects those with permanent urethral catheters, it has also been documented in patients with percutaneous nephrostomy and suprapubic catheters1,4.
Global data from 2017 reported a mean patient age of 76.7 years, with a significant female predominance (70.9%). Common risk factors identified were being bedridden (66.1%), institutionalization (67.1%), dementia (42.4%), constipation (53.6%), and alkaline urine (69.9%)4. In contrast, a 2023 observational study from India reported a younger mean age of 67.4 years and a male predominance (67.4%). Despite these demographic differences, the clinical profile remained consistent with a high prevalence of chronic constipation (73.9%) and alkaline urine (93.5%)1.
Current literature indicates that 59.4% to 76.1% of patients presenting with PUBS are asymptomatic1,4. While the overall prognosis is generally favourable, severe complications have been documented, including nine deaths and two cases of Fournier's gangrene among 117 cases4. Consequently, the consensus among authors is that the need for antibiotic therapy must be assessed on an individual basis, prioritizing those with systemic symptoms or high risk for complications1,4. Other aspects of management include replacing the catheter, managing constipation, and reinforcing strict genitourinary hygiene and catheter care1,3,4.
Although our patient is a young adult, he possessed significant risk factors, including chronic catheterization, immobility and intermittent constipation. While PUBS is typically associated with the elderly, it has also been reported in younger populations3,7. Although urinary pH was not documented in his initial urine sample, it was found to be acidic on the fourth day of admission. Notably, his urine culture identified Staphylococcus aureus, a relatively uncommon but previously reported causative organism in cases of PUBS8,9. Furthermore, our patient was symptomatic, in contrast to the majority of patients with PUBS. His outcome was favourable following prompt clinical assessment and initiation of appropriate management. This case underscores the importance of recognizing PUBS in younger, symptomatic patients and its association with Staphylococcus aureus, a Gram-positive coccus.
CONCLUSION
PUBS can indicate an underlying urinary tract infection in patients on long-term urinary catheters. Although often benign, it can lead to unfavourable outcomes if overlooked by healthcare providers who are unaware of the phenomenon. Awareness of this condition is vital to ensure prompt recognition, appropriate clinical assessment and targeted management.
INFORMED CONSENT
Informed written consent was obtained from the patient.
No identifying patient information or photographs that could lead to patient identification are presented.
ACKNOWLEDGEMENT
We thank the patient for providing consent to publish this case report.
REFERENCES
1. Neniwal VK, Swain S, Rulaniya SK, Hota D, Agarwal P, Yadav PK. Purple urine bag syndrome: An unusual manifestation of urinary tract infection, our experience at a tertiary care center. Curr Urol. 2023 Jun;17(2):125-9. [PubMed] [Full Text] [DOI]
2. Dealler SF, Hawkey PM, Millar MR. Enzymatic degradation of urinary indoxyl sulfate by Providencia stuartii and Klebsiella pneumoniae causes the purple urine bag syndrome. J Clin Microbiol. 1988 Oct;26(10):2152-6. [PubMed] [Full Text] [DOI]
3. Khan F, Chaudhry MA, Qureshi N, Cowley B. Purple urine bag syndrome: an alarming hue? A brief review of the literature. Int J Nephrol. 2011 Oct;2011:419213. [PubMed] [Full Text] [DOI]
4. Llenas-Garcia J, Garcia-Lopez M, Perez-Bernabeu A, Cepeda JM, Wikman-Jorgensen P. Purple urine bag syndrome: A systematic review with meta-analysis. Eur Geriatr Med. 2017 Jul;8(3):221-7. [Full Text] [DOI]
5. Saraireh M, Gharaibeh S, Araydah M, Al Sharie S, Haddad F, Alrababah A. Violet discoloration of urine: A case report and a literature review. Ann Med Surg (Lond). 2021 Jul 16;68:102570. [PubMed] [Full Text] [DOI]
6. Barlow GB, Dickson JAS. Purple urine bags. Lancet. 1978 Jan;311(8057):220-1. [Full Text] [DOI]
7. Jappi Y, Hadi U. Purple Urine Bag Syndrome in Urinary Tract Infection. J Glob Infect Dis. 2023 Mar 31;15(2):84-5. [PubMed] [Full Text] [DOI]
8. Vaidyanathan S, Soni BM. Bluish discolouration of urine drainage tube and bag in a female patient with spina bifida, paraplegia, and suprapubic cystostomy. ScientificWorldJournal. 2007 Jul 3;7:1070-2. [PubMed] [Full Text] [DOI]
9. Mantani N, Ochiai H, Imanishi N, Kogure T, Terasawa K, Tamura J. A case-control study of purple urine bag syndrome in geriatric wards. J Infect Chemother. 2003 Mar;9(1):53-7. [PubMed] [Full Text] [DOI]
|
AUTHORS CONTRIBUTION |
|
Following authors have made substantial contributions to the manuscript as under: |
|
KT: Conceptualization, literature review, editing, reviewing and original article |
|
KZ: Literature review, editing, reviewing and original article |
|
TZ: Literature review, editing, reviewing and original article |
|
Authors agree to be accountable for all respects of the work in ensuring that questions related to the accuracy and integrity of any part of the work are appropriately investigated and resolved. |
|
CONFLICT OF INTEREST |
|
None |
|
GRANT SUPPORT AND FINANCIAL DISCLOSURE |
|
None |