CASE REPORT
https://doi.org/10.47811/bhj.198
Periorbital varicella gangrenosa, rare complication of chickenpox: a case report
Samten Dorji 1, Sonam Jamtsho2, Dechen Wangmo1, Sonam3
1Department of Ophthalmology, Jigme Dorji Wangchuck National Referral Hospital, Thimphu, Bhutan
2Department of Surgery, Jigme Dorji Wangchuck National Referral Hospital, Thimphu, Bhutan
3Department of Paediatrics, Jigme Dorji Wangchuck National Referral Hospital, Thimphu, Bhutan
Corresponding author:
Samten Dorji
samtend@jdwnrh.gov.bt
ABSTRACT
Periorbital varicella gangrenosa is an extremely rare and severe complication of varicella infection, with limited literature describing periorbital involvement. We report the first documented case from Bhutan involving a 4-year-old female child who presented with bilateral eyelid swelling, more severe on the left eye, following a recent varicella infection. A clinical diagnosis of left periorbital varicella gangrenosa was confirmed. The patient was managed through a multidisciplinary approach and underwent serial surgical debridement followed by split-thickness skin grafting. Despite extensive tissue loss due to delayed presentation, effective infection control was achieved, vision was preserved, and a satisfactory cosmetic outcome was obtained, although residual lagophthalmos persisted. This case highlights the importance of early recognition and aggressive multidisciplinary management to prevent severe morbidity and mortality.
Keywords: Eyelids; Necrotizing Fasciitis; Varicella gangrenosa
INTRODUCTION
Varicella, commonly known as chickenpox, is caused by the varicella zoster virus (VZV) and affects an estimated 84 million cases annually, predominantly children1. Chickenpox is a highly contagious viral disease transmitted via inhalation of aerosolized respiratory droplets. It is classically characterized by the sequential eruption of pruritic erythematous macules and papules that typically begin on the head and face and subsequently disseminate to the trunk and extremities. The diagnosis of varicella infection is predominantly clinical, based on characteristic signs and symptoms, and its management ranges from supportive symptomatic care to antiviral therapy depending on disease severity and patient risk factors2.
Varicella can cause periorbital varicella gangrenosa which is an extremely rare complication with a prevalence rate of 0.05-0.16%. Periorbital infections can lead to significant morbidity resulting in vision loss and facial disfigurement. There is limited literature available on its presentation and management3. We present a case of a 4-year-old female child with periorbital varicella gangrenosa involving the left side periorbita, who required multiple surgical debridement and subsequent skin grafting at the National Eye Center, managed through a multidisciplinary approach.
PATIENT INFORMATION
A 4-year-old female child presented to the National Eye Center with a 5-day history of bilateral eyelid swelling, more pronounced on the left side. The ocular symptoms were preceded by a recent episode of varicella infection, manifesting as erythematous macules and papules over the face, which appeared two days prior to the onset of eyelid swelling. She was initially evaluated at the emergency department of Jigme Dorji Wangchuck National Referral Hospital (JDWNRH) on the day the swelling began and was commenced on oral antibiotics. However, the patient was subsequently lost to follow-up and re-presented to the National Eye Center on day five with progressively worsening bilateral eyelid oedema.
CLINICAL FINDINGS
On general examination, the child was conscious, alert, and cooperative for her age. She was haemodynamically stable. Systemic examination was unremarkable. Cutaneous examination revealed few crusted varicella lesions over the face and trunk, with no active vesicular eruptions.
Ocular examination of the right eye showed mild eyelid oedema without erythema or tenderness. The conjunctiva, cornea, anterior chamber, and pupillary reactions were within normal limits. The left eye showed marked eyelid oedema and erythema with areas of necrosis involving both the upper and lower eyelids, associated with mucopurulent discharge. Tissue loss was more pronounced in the upper eyelid region (Figure 1). Conjunctival chemosis was present. The globe was intact, and the cornea was clear. Visual acuity and extraocular movements could not be adequately assessed due to pain and severe lid oedema. There were no clinical signs of orbital involvement such as proptosis.

Figure 1. Patient’s left eye at the time of presentation
DIAGNOSTIC ASSESSMENT
Computed tomography demonstrated left eye pre-septal necrotising fasciitis extending to the left temporo-frontal-parietal scalp (Figure 2). The patient was diagnosed with periorbital varicella gangrenosa of the left eye, complicated by secondary bacterial infection and necrotising fasciitis. Baseline laboratory investigations revealed neutrophilic leukocytosis, a C-reactive protein level of 164 mg/L and an erythrocyte sedimentation rate of 62 mm/hr. Blood cultures were obtained prior to initiation of intravenous antibiotics and showed no growth.
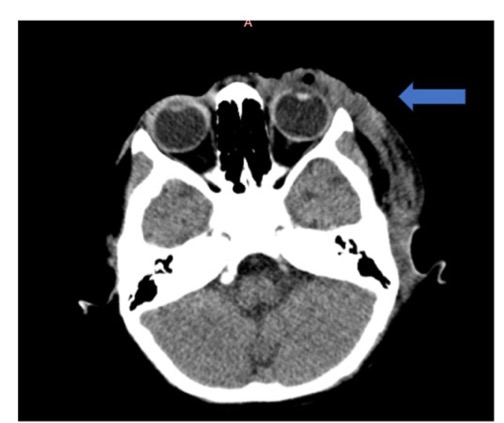
Figure 2. Non-contrast axial CT scan of the orbit showing extensive left preseptal soft-tissue swelling with collections and air locules extending to the left temporo-frontal-parietal scalp.
The patient was admitted under the Department of Paediatrics for inpatient management. She was empirically started on intravenous ceftriaxone, a broad-spectrum antimicrobial agent, before undergoing surgical debridement. Antibiotic therapy was later continued based on tissue culture and sensitivity results.
THERAPEUTIC INTERVENTION
Wound debridement was performed under general anaesthesia at JDWNRH by a multidisciplinary team comprising an oculoplastic surgeon and a plastic surgeon. Debrided tissue was sent for histopathological examination and culture. Intraoperatively, left eye upper conjunctival chemosis was noted, while the cornea was clear and fundus was unremarkable. Periorbital necrosis involved both the upper and lower eyelids, extending to the upper brow and 1-2 cm lateral to the lateral canthus. In depth, it affected the orbicularis muscle of both the upper and lower eyelid, while sparing the tarsus. Extensive debridement was done involving a 2 mm margin of healthy skin and muscle. A temporary tarsorrhaphy was performed to protect the ocular surface. A repeat debridement was performed after 3 days for adequate infection control and to prepare the wound bed for subsequent skin grafting (Figure 3).

Figure 3. (a) Intraoperative debridement. (b) After first debridement showing necrotic tissue (c) After second debridement showing healthy granulation tissue
Tissue biopsy revealed features consistent with necrotizing fasciitis and cultures yielded a positive growth of Streptococcus pyogenes and Staphylococcus aureus. Both organisms were sensitive to cephalosporins therefore the patient was continued on intravenous ceftriaxone as started on first day of admission.
The patient was transferred to the Paediatric Intensive Care Unit for close observation and was subsequently transferred to the Paediatric Ward once clinically stable. During inpatient management, she was started on intravenous acyclovir as well.
One week after the second debridement, the patient was handed over to the plastic and reconstructive surgeon for defect coverage. A full thickness skin graft measuring 2x4 cm was harvested from the right groin and sutured over the wound bed using 6-0 polypropylene suture (Figure 4). The wound dressing was done with Petroleum Jelly and betadine. Graft assessment was performed under general anaesthesia one week later, demonstrating good graft uptake. Sutures were removed under sedation at two weeks. Post operatively, the graft was regularly moisturised and massaged with neomycin for the first two weeks, followed by twice-daily application of coconut oil.
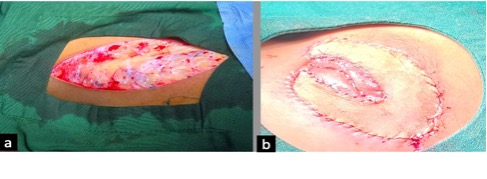
Figure 4. (a) Split-thickness skin graft harvested from the right inguinal region. (b) The graft was appropriately positioned and anchored to the recipient bed.
FOLLOW – UP AND OUTCOMES
The patient was followed up weekly for the first month, followed by three-monthly visits over the subsequent year. At follow-up, visual acuity was 6/6 in both eyes, with the left eye achieving 6/6 after myopic correction. At the three-month review, the graft demonstrated good uptake although lagophthalmos was noted, for which lubricating eye medications were prescribed (Figure 5).
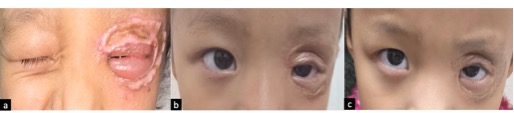
Figure 5. (a) One-month postoperative follow-up demonstrating a well-integrated graft with residual lagophthalmos. (b) Three-months postoperative follow up. (c) Six-months postoperative follow up
DISCUSSION
Periorbital necrotizing fasciitis is a rare but dreaded complication of varicella, typically occurring during the convalescent phase of varicella, when vesicular lesions begin to crust, acting as a portal of entry for secondary bacterial infection4. Early recognition and prompt, aggressive management is required to prevent devastating complications such as vision loss, facial disfigurement and mortality. Historically described as varicella gangrenosa by Stokes in 1807, this condition is most commonly associated with subcutaneous streptococcal infection4,5. Reported cases highlight its potential severity, including immunocompetent patients progressing to develop periorbital necrotizing fasciitis, requiring orbital exenteration and ultimately dying due to complications6.
Clinically, patients present with rapidly progressive periorbital swelling, erythema, severe pain disproportionate to local findings, purulent discharge, and skin necrosis often accompanied by systemic features ranging from fever to sepsis3. Local examination may reveal eyelid oedema, erythema, skin discolouration, and necrosis. Thorough ocular assessment is essential to assess globe integrity, identify signs of orbital involvement and differentiate from conditions such as preseptal cellulitis, orbital cellulitis and other causes of periorbital inflammation. These distinctions are important as delay in diagnosis may lead to vision loss or mortality6.
Diagnosis is primarily clinical, supported by elevated inflammatory markers, including C-reactive protein and erythrocyte sedimentation rate4. Computed tomography of the orbit is the preferred supportive imaging modality of choice to delineate the disease extent and guide surgical planning3. Definite confirmation is achieved through histopathological examination and microbiological culture of debrided tissue. It also allows targeted antimicrobial therapy4.
Early recognition of complication of varicella and initiating management including antibiotics and wound debridement can reduce morbidity, disfigurement and mortality. Furthermore, a multidisciplinary approach involving paediatric ophthalmologist, oculoplastic surgeon, paediatrician, infectious disease specialist and plastic surgeon can optimize outcomes5.
In our case, although these principles guided management, there was a delay in definitive intervention. The patient was initially advised early review but presented only on the fifth day after the onset of complications, by which time significant periorbital tissue necrosis had developed. Consequently, surgical debridement resulted in extensive tissue loss requiring reconstruction with a split-thickness skin graft. Despite the delay, prompt multidisciplinary management helped achieve key treatment goals that included the prevention of further spread of infection, preservation of vision, maintaince of eyelid function and acceptable cosmetic outcome.
Currently, the child has lagophthalmos but no exposure keratopathy and remains under regular follow-up. The case reinforces the critical importance of early recognition, strict follow-up and timely surgical intervention in varicella patients, along with effective counselling of caregivers regarding potential complications to ensure timely healthcare seeking behaviour.
CONCLUSION
This case emphasizes the importance of maintaining a high index of suspicion for periorbital varicella gangrenosa in children presenting with rapidly progressive periorbital swelling following varicella infection. Timely recognition, early imaging, aggressive surgical debridement, and a multidisciplinary approach are critical to reducing the risk of severe morbidity, vision loss, and mortality.
INFORMED CONSENT
Informed written consent was obtained from the patient’s guardian, along with assent from the patient. This included permission to use clinical images for publication.
ACKNOWLEDGEMENT
The authors acknowledge the contributions of the Departments of Ophthalmology, Paediatrics, and Surgery at the JDWNRH in the management of this case.
REFERENCES
1. Wooding EL, Kadambari S, Warris A. Varicella: is it time for a global vaccination programme? Arch Dis Child. 2025;110(8):586-91.[PubMed] [DOI]
2. Saleh HM, Ayoade F, Kumar S. Varicella-zoster virus (chickenpox). [Updated 2025 Apr 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448191/
3. Jain J, Thatte S, Singhai P. Periorbital varicella gangrenosa: A rare complication of chicken pox. Oman J Ophthalmol. 2015;8(1):64-6. [PubMed] [Full Text] [DOI]
4. Wilson GJ, Talkington DF, Gruber W, Edwards K, Dermody TS. Group A streptococcal necrotizing fasciitis following varicella in children: case reports and review. Clin Infec Dis. 1995;20(5):1333-8.[PubMed] [DOI]
5. Stokes W. On an eruptive disease of children. Med Phys J. 1808;19(110):344-50. [PubMed] [Full Text]
6. Thomas WO, Parker JA, Weston B, Evankovich C. Periorbital varicella gangrenosa necessitating orbital exenteration in a previously healthy adult. South Med J. 1996;89(7):723-5. [PubMed] [DOI].
|
AUTHOR CONTRIBUTIONS SD: Concept, design, literature search, manuscript writing, editing SJ: Concept, design, literature search, manuscript writing, editing DW: Concept, design, literature search, manuscript writing, editing S: Concept, design, literature search, manuscript writing, editing Authors agree to be accountable for all respects of the work in ensuring that questions related to the accuracy and integrity of any part of the work are appropriately investigated and resolved.
|
|
CONFLICT OF INTEREST None
GRANT SUPPORT AND FINANCIAL DISCLOSURE None
|