ORIGINAL ARTICLE
https://doi.org/10.47811/bhj.203
Awareness and Practices among Patients with Allergic Rhinitis Receiving Intranasal Corticosteroid Spray at National Referral Hospital, Bhutan: A Cross Sectional Study
Sonam Jamtsho1,2, Sonam Chhoden R3, Dorji Pelzom4, Santosh Mukhia1,2
1Department of Ear Nose and Throat, Jigme Dorji Wangchuk National Referral Hospital, Bhutan
2Faculty of Post graduate Medicine, Khesar Gyalpo University of Medical Sciences of Bhutan
3Faculty of Undergraduate Medicine, Khesar Gyalpo University of Medical Sciences of Bhutan
4Ministry of Health, Bhutan
Corresponding author:
Dr. Sonam Jamtsho
INTRODUCTION
Allergic rhinitis is a common chronic inflammatory disorder of the nose and paranasal sinuses, affecting approximately 10–40% of the adult population worldwide and an estimated 500 million individuals globally1. Its prevalence and associated healthcare burden are increasing, becoming a major global public health concern2. Environmental and lifestyle factors, including air pollution, poor indoor ventilation, overcrowding, tobacco exposure, and sedentary behavior, have been implicated in this rising trend3,4. In Asia, prevalence rates range from 27% in South Korea to 32% in the United Arab Emirates5.
Despite its global burden, data on the prevalence and clinical impact of allergic rhinitis in Bhutan are limited. To date, no population-based epidemiological studies have been conducted in the country. Retrospective review of ENT outpatient records at JDWNRH for the year 2020 indicates that approximately 10–15% of patients presented with symptoms consistent with allergic rhinitis. These findings underscore the clinical relevance of allergic rhinitis in the Bhutanese population and highlight the need for systematic evaluation of patients’ awareness and practices regarding the disease and its management.
Allergic rhinitis is a non-communicable, IgE-mediated inflammatory condition of the nasal mucosa and paranasal sinuses, characterized by nasal obstruction, paroxysmal sneezing, rhinorrhea, and nasal irritation6. Therapeutic strategies encompass pharmacological and immunomodulatory approaches, including oral and intranasal antihistamines, intranasal corticosteroids, and allergen-specific immunotherapy. Intranasal corticosteroids are the recommended first-line therapy and have demonstrated superior efficacy compared with oral and intranasal antihistamines in controlling overall nasal symptoms1,3,6–8. In addition to pharmacotherapy, allergen avoidance and correct intranasal spray technique are essential for optimal disease control9–11.
Inadequate patient awareness has been associated with poor treatment adherence, suboptimal practices, and inadequate symptom control12–15. Given the chronic nature of allergic rhinitis and the importance of long-term therapy, patient knowledge and practices play a critical role in treatment outcomes13,16–18. This study aims to assess awareness and practices among patients with allergic rhinitis receiving intranasal corticosteroids spray at the ENT OPD, JDWNRH.
METHODS
Study design
A cross-sectional study was conducted at the ENT Department, of the JDWNRH, Bhutan from 01st July 2022 to 31st Jan 2023.
Study setting
The ENT department consists of five consultation chambers. Chambers 1–4 are each staffed by an ENT consultant supported by an ENT technician and provide routine outpatient clinical services. Chamber 5 functions as a dedicated screening unit for walk-in patients and is staffed by ENT technicians who provide basic ENT services and minor procedural services, including wound dressing, cerumen removal, and suture removal.
The department maintains an inpatient ENT ward located on the third floor of the hospital, with a total capacity of 18 beds, accommodating both male and female patients requiring inpatient care. Surgical services are routinely conducted in Operation Theatre (OT)-7 six days per week. During the study period, the department was staffed by six ENT surgeons, four postgraduate residents, twelve ENT technicians, four audiologists, thirteen nursing staff, and one receptionist.
All patients attending the ENT outpatient services consulted ENT specialists through a prior appointment obtained at the reception counter. Direct walk-in patients were initially screened by ENT technicians at Chamber 5 and were advised to obtain an appointment for consultant evaluation when indicated.
Study population
All patients coming with symptoms of allergic rhinitis to the ENT department
Inclusion Criteria
All patients aged 18 years and above who were diagnosed with allergic rhinitis and provided consent to participate were included in the study.
Exclusion criteria
Patients under 18 years of age, those with allergic rhinitis not using intranasal corticosteroid spray, and those with non-allergic rhinitis-including chronic rhinosinusitis (CRS), nasal polyps, and vasomotor rhinitis-were excluded from the study.
Sample size calculation
The required sample size (n) was calculated using the single population proportion formula.
n=(p(1-p)*Z^2)/e^2
A proportion (p) of 0.72 was used based on previous studies showing that about 72% of patients had poor awareness and practice regarding allergic rhinitis and its treatment (19). With a 95% confidence level (Z = 1.96) and a margin of error of 5% (e = 0.05), the final calculated sample size was 188 participants.
Sampling technique
Study participants were selected using systematic random sampling. The first patient was chosen randomly by a lucky draw from the numbers 1, 2, and 3, with number 2 drawn. Thus, the second patient diagnosed with allergic rhinitis on the first day of data collection was included as the first participant. Thereafter, every second patient meeting the inclusion criteria was systematically included in the study.
Study procedure
All patients visiting ENT OPD were screened for allergic rhinitis, and those diagnosed with allergic rhinitis were directed to the investigators for collection of data and assessment of technique of nasal spray application.
To assess correct nasal spray technique, patients were requested to demonstrate the spraying technique using an empty spray bottles according to the seven-step method outlined by Beninger MS et al20. Regular follow-up attendance is an important practice indicator for patients receiving long-term treatment with intranasal corticosteroid sprays. Accordingly, adherence to advised follow-up was assessed retrospectively through a review of departmental outpatient Google Sheet records maintained by the department at 4-6 weeks interval after the initial visit. All these data were collected using a study questionnaire.
Regular follow-up attendance is an important practice indicator for patients receiving long-term treatment with intranasal corticosteroid sprays. Accordingly, adherence to advised follow-up was assessed retrospectively through a review of departmental outpatient Google Sheet records maintained by the department at 4-6 weeks interval after the initial visit.
Study tool
The research questionnaire was developed using references from the previous KAP studies on Allergic rhinitis19,21–23. The questionnaires were adapted with minor contextual modifications to ensure appropriateness for the Bhutanese population. Content validation was performed through expert review by a panel of three ENT surgeons and an ENT technician at the National Referral Hospital. Content validity was quantified using the Content Validity Index (CVI), with all items achieving a CVI of 0.80, indicating acceptable content validity. Subsequently, pilot testing was conducted among 20 patients attending the ENT OPD to evaluate clarity, feasibility, and comprehensibility. The questionnaires were found to be unambiguous, easily understood by respondents, and required only a short time to complete.
There were six questions to assess the awareness levels and four questions to assess the practice. Each correct response to the awareness questions was awarded one mark, while incorrect or equivocal responses received zero marks. Of a maximum possible score of six, participants scoring four or more (70%) were classified as having good awareness, and vice versa. Similarly, each appropriate practice was awarded one mark, with no marks assigned for inappropriate practices. Out of a maximum score of four, participants scoring three or more (70%) were categorized as having good practice and vice versa14,15,24.
Data variables
Socio-demographic variables (age, gender, education, occupation, and address), awareness or knowledge about allergic rhinitis and its treatment and their practice towards the treatment of allergic rhinitis were collected using a validated questionnaire.
Statistical analysis
Data was recorded using EpiData 3.1 software and then exported in stata.dta format and statistical analysis was performed using StataCorp Stata 14.2 2 (StataCorp LLC, College Station, TX, USA). Descriptive analysis of the demographic data was presented as frequency and percentage. Association between socio-demographic factors to the levels of awareness and practice (good/poor) were done using a univariable and multivariable logistic regression analysis. Odds ratios along with 95% confidence interval (95%CI) are presented as appropriate. P-value of <0.05 is considered as significant.
Ethical statement
Ethical clearance to conduct the study was sought from IRB letter no: Ref. No. IRB/Approval/PN21-017/2021/519. Administrative clearance sought from MoH and site clearance was sought from JDWNRH. Written informed consents were taken from all the patients before the data collection. Data were annonymised before the data analysis.
RESULTS
Sociodemographic characteristics
A total of 201 patients were interviewed and assessed for awareness and practice. Over 74% of them were in the age range of 25-44 years, and majority of them were female (63%). Table 1 summarizes the demographics of the study subjects who participated in this study.
Table 1: Socio-demographic characteristics of study subjects with allergic rhinitis on intranasal corticosteroid at the ENT Department of JDWNRH, 2022-2023, (n=201).
|
Characteristics |
n (%) |
|
|
Age (Years) |
18-24 |
32 (16) |
|
25-34 |
73 (36) |
|
|
35-44 |
76 (38) |
|
|
>45 |
20 (10) |
|
|
Mean age (SD) |
33.6 (9) |
|
|
Gender |
Male |
74 (37) |
|
Female |
127 (63) |
|
|
Education |
No formal education |
24 (12) |
|
Up to higher secondary |
48 (24) |
|
|
Post-Secondary(TVET and Diploma) |
65 (32) |
|
|
Bachelors and above |
64 (32) |
|
|
Occupation |
Unemployed |
58 (29) |
|
Technician/Associate |
47(23) |
|
|
Skilled worker |
42 (21) |
|
|
Professional/Managerial |
54 (27) |
|
|
Present address |
West |
185 (95) |
|
Central |
9 (5) |
|
|
East |
7 (3) |
|
|
Permanent address |
West |
75 (37) |
|
Central |
56 (28) |
|
|
East |
70 (36) |
|
From the four cardinal symptoms of allergic rhinitis, all patients presented with nasal obstruction (100%) followed by recurrent sneezing (81%), and nasal irritation as illustrated in Figure 1.
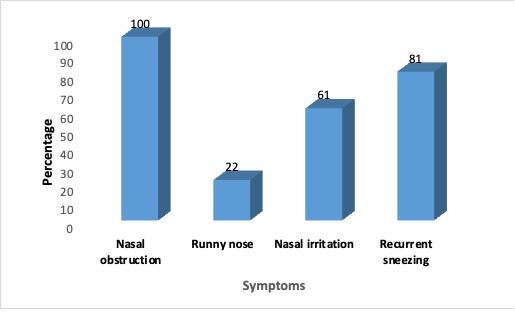
Figure 1: Illustrates symptom analysis of the patients with allergic rhinitis at the ENT OPD JDWNRH, 2022-223, (n=201).
Awareness about allergic rhinitis and treatment
Awareness level among the patients were poor in majority of them (71%, n=142). Only 48% (n=96) of the patient knew that allergic rhinitis is a non-contagious disease. Though majority of the patient were aware that life style and environment did affect their allergic symptoms (74%, n=148), only 22% (n=45) knew that allergic rhinitis can be prevented. Only few patients knew that the nasal spray they were using contained steroids while 44% (n=88) didn’t know it should be used for a longer duration as shown in table 2.
Table 2: Proportion of study participants with allergic rhinitis receiving intranasal corticosteroid spray aware about the disease and treatment at the ENT OPD JDWNRH, 2022-2023, (n=201).
|
Awareness questions |
Yes |
No |
Don't Know |
Not sure |
|
n(%) |
n(%) |
n(%) |
n(%) |
|
|
Allergic rhinitis is a contagious infection of nose. |
30(15) |
⃰ 97(48) |
69(34) |
5(2) |
|
Life style, diet and environment affects allergic rhinitis. |
⃰ 153(74) |
12(6) |
34(17) |
2(1) |
|
Allergic Rhinitis can be prevented. |
⃰ 44(22) |
27(13) |
128(64) |
2(1) |
|
Allergic Rhinitis tends to run in families. |
⃰ 108(52) |
36(18) |
55(27) |
2(1) |
|
Nasal spray contains steroids |
⃰ 12(6) |
9(4) |
166(83) |
14(7) |
|
Nasal steroid spray should be applied for at least 6 weeks. |
⃰ 118(59) |
5(2) |
76(40) |
2(1) |
|
Awareness levels |
Frequency |
|
Percentage |
|
|
ℷ Good Awareness |
59 |
|
29 |
|
|
Poor Awareness |
142 |
|
71 |
|
⃰ Indicates correct responses. ℷ Good awareness are those scoring >=4, Poor awareness are those scoring<4
Practice and technique of spray application
From 201 patients, 55% (n=111) of the subjects exhibited poor practice. Only 47% (n=94) of the patients used nasal spray as prescribed showing a poor compliance to treatment while 66% (n=132) do visit doctors when they get the nasal symptoms. In more than half of the study subjects their technique of nasal spray application was incorrect (n=115) as shown in Table 3.
Table 3: Proportion of study participants with allergic rhinitis receiving intranasal steroid spray and their practice patterns and the technique of spray application at the ENT OPD, JDWNRH, 2022-2023,(n=201).
|
Practice Questions |
Yes |
No |
|
n (%) |
|
|
|
|
|
n (%) |
|
I use nasal steroid spray without fail as prescribed. |
94(47) |
107(53) |
|
I avoid dust and smoke. |
183(91) |
18(9) |
|
I visit doctor whenever I get symptoms of allergic rhinitis |
132(66) |
69(34) |
|
Did the patient turn up for follow-up at one month |
59(29) |
142(71) |
|
Practice levels |
Frequency |
Percentage |
|
ℷ Good Practice |
90 |
45 |
|
Poor Practice |
111 |
55 |
|
|
Correct |
Not Correct |
|
Technique of Nasal spray application |
n(%) |
n(%) |
|
Demonstrated the technique of applying the nasal steroids |
86(43) |
115(57) |
ℷ Good practices are those scoring >=3, Poor practice are those scoring<3
Logistic regression analysis revealed that female patients were 2.1 times more likely to demonstrate better awareness regarding allergic rhinitis and treatment (aOR 2.1, 95%CI 1.52 - 4.57, p=0.002). Furthermore, those who have attained better education were significantly at higher odds of having better awareness as compared to those who didn’t receive any formal education as shown in Table 4.
Table 4: Logistic regression analysis showing association between socio-demographic factors and the awareness about disease and treatment among patients with allergic rhinitis receiving intranasal corticosteroid spray at JDWNRH, 2022-2023, (n=201).
|
Awareness |
|
cOR (95% CI) |
p-value |
aOR (95% CI) |
p-value |
|
Gender |
Male (Ref) |
|
|
|
|
|
|
Female |
2.3(1.6 - 4.4) |
0.001 |
2.1(1.5 - 4.5) |
0.002 |
|
Age |
18-24 (Ref) |
|
|
|
|
|
|
25-35 |
1.3(0.8 - 3.2) |
0.263 |
1.4(0.8- 2.3) |
0.173 |
|
|
35-45 |
1.1(0.6 - 1.7) |
0.652 |
1.2(0.7 - 2.1) |
0.497 |
|
|
>45 |
1.5(0.9 - 2.6) |
0.091 |
1.5(0.8 - 2.2) |
0.181 |
|
Education |
No Formal education (Ref) |
|
|
|
|
|
|
Up to higher secondary |
1.3(0.8 - 2.18) |
0.331 |
1.3(0.9 - 2.6) |
0.282 |
|
|
TVET / Diploma |
1.7( 1.2- 3.2) |
0.022 |
1.8(1.3 – 3.6) |
0.026 |
|
|
Bachelors and above |
2.9(1.6- 4.3) |
0.001 |
2.7(1.3 – 3.7) |
0.001 |
|
Occupation |
Unemployed (Ref) |
|
|
|
|
|
|
Technician/Associate |
1.1(0.5 - 1.5) |
0.533 |
1.3(0.6 - 1.8) |
0.265 |
|
|
Skilled worker |
1.3(0.8 - 2.1) |
0.294 |
1.2(0.7 - 2.0) |
0.475 |
|
|
Managerial/ Professional |
1.9(1.4– 4.4) |
0.021 |
1.5(1.2 - 3.3) |
0.081 |
|
⃰Regions |
West (Ref) |
|
|
|
|
|
|
Central |
1.1(0.8 - 2.1) |
0.632 |
- |
- |
|
|
East |
1.1(0.7 – 1.8) |
0.816 |
- |
- |
cOR: Crude odds ratio, aOR: Adjusted odds ratio, CI: Confidence interval. Ref: Reference category for comparison, TVET: Technical and vocational education and training
⃰ Region was not modelled into the Multivariable logistic regression as none of the p-value were below 0.2.
Statistical analysis revealed that practice levels were not significantly associated with sociodemographic variables or with the technique of intranasal corticosteroid application across patient subgroups (Table 5).
Table 5: Logistic regression analysis showing association between socio-demographic factors and the practice level among patients with allergic rhinitis receiving intranasal steroid spray at JDWNRH, 2022-2023, (n=201).
|
Practice |
|
cOR (95% CI) |
p-value |
aOR(95%CI) |
p-value |
|
Gender |
Male(Ref) |
|
|
|
|
|
|
female |
0.9(0.9 - 1.8) |
0.891 |
0.8(0.8 - 1.7) |
0.415 |
|
Age |
18-24(Ref) |
|
|
|
|
|
|
25-35 |
1.3(0.8 - 2.4) |
0.203 |
1.1(0.7 - 2.1) |
0.693 |
|
|
35-45 |
1.3(0.7 - 2.1) |
0.294 |
1.2(0.6 - 1.8) |
0.433 |
|
|
>45 |
0.9(0.6 - 1.5) |
0.819 |
1.2(0.8 - 2.3) |
0.377 |
|
Education |
No Formal education (Ref) |
|
|
|
|
|
|
Up to higher secondary |
1.2(0.8 - 2.2) |
0.353 |
1.2(0.7 - 1.9) |
0.412 |
|
|
TVET / Diploma |
1.4(0.8 - 2.4) |
0.295 |
1.3(0.8 - 2.3) |
0.236 |
|
|
Bachelors and above |
1.5(0.9 - 2.6) |
0.098 |
1.6(0.8 - 2.5) |
0.071 |
|
Occupation |
Unemployed (Ref) |
|
|
|
|
|
|
Technician/Associate |
1.1(0.6 - 1.6) |
0.562 |
0.9(0.5 -1.6) |
0.835 |
|
|
Skilled worker |
1.3(0.7 - 2.1) |
0.254 |
1.1(0.7 - 2.0) |
0.592 |
|
|
Managerial/ Professional |
1.6(0.9 - 2.8) |
0.065 |
1.4(0.9 -2.7) |
0.139 |
|
⃰ Regions |
West (Ref) |
|
|
|
|
|
|
Central |
1.1(0.7 - 2.2) |
0.492 |
- |
- |
|
|
East |
1.2(0.8 - 2.3) |
0.397 |
- |
- |
cOR : Crude odds ratio, aOR : Adjusted odds ratio, CI: Confidence interval, Ref: Reference category for comparison, TVET: Technical and vocational education and training
⃰ Region was not modelled into the Multivariable logistic regression as none of the p-value were below 0.
DISCUSSION
In this study, 71% (n=142) of patients demonstrated poor awareness of allergic rhinitis and its management. Although most participants recognized the influence of lifestyle and environmental factors on symptoms, less than a quarter were aware that the allergic rhinitis can be prevented. This finding is clinically relevant, as patient education and allergen avoidance are central to effective management of allergic rhinitis3,6,9,25.
Logistic regression analysis identified educational attainment as a significant determinant of awareness level. Higher educational status was associated with progressively increased odds of good awareness, with a statistically significant association observed among participants holding a post-secondary education and. Additionally, individuals employed in professional or managerial roles demonstrated significantly greater awareness, a relationship that likely reflects the influence of higher educational exposure status. The findings of this study are consistent with the study done by Corbett et al. who also reported similar association between education attainment and awareness18.
Notably, female participants exhibited 2.1-fold higher odds of good awareness compared with males, suggesting potential sex-based differences in health information–seeking behavior and engagement with disease-related knowledge. However, studies done in other countries reveal males were better aware about the disease and treatment as compared to females which they attributed to difference in education status between the genders in their countries14,19. These observations demonstrate the critical role of education of patients on the disease awareness and thus a targeted education program forms an integral component of allergic rhinitis management3,25,26.
In this study, 55% (n=201) of patients exhibited suboptimal treatment practices. Adherence to prescribed intranasal corticosteroid therapy was observed in only 47% (n=94) participants, 29% (n=58) attended one-month follow-up visits, and 34% failed to seek medical care despite persistent allergic symptoms. These findings are consistent with previous KAP studies conducted globally13–15,19, which attributed poor treatment practices to limited disease knowledge and misperceptions, a finding which is also evident in our study. Although this study didn’t asses why the compliance to treatment was poor, study done by Bridgeman MR, 2017, the reasons for poor compliance were due to safety issues, misperceptions regarding the loss of response from frequent use, and undesirable sensations associated with intranasal administration10,27.
Among the study subjects 57% (n=115) demonstrated incorrect technique, with the majority failing to prime the spray correctly and neglecting to clear the nasal passages prior to application. The reason might be due to poor counselling and demonstration of use of intranasal corticosteroid spray. Study done in Europe and around revealed that patient training forms an integral part of management of allergic rhinitis10,13,26–28.
Although higher educational attainment was significantly associated with greater awareness, this did not translate into improved treatment practices. The gap between knowledge and practice may reflect insufficient patient counseling and education in high-volume outpatient settings. These findings emphasizes the need for structured, targeted education programs to enhance disease understanding and ensure correct use of therapy, thereby optimizing allergic rhinitis management.
From the 201 study subjects, 63% were females and 37% were males. There is female predominance in the number of patients who visited during the study period which is in concurrence with similar studies done around the globe29,30. Majority (88%) of the study subjects were from the young adult age group between 18-45 years of age which could be explained by higher preponderance for activities and exposure in this age group. An international survey study done by Barghav et.al also found similar age ranges except for South Korea and Japan where the majority of the subjects were younger than 18 years and older than 50 respectively5.
Among the three regions in Bhutan, most of patients came from western region because the site of study was in JDWNRH which is located in the western region. Also it could be because western region is the most develop with majority of the economic activity happening in the western region as allergic rhinitis is found to be more prevalent in higher socioeconomic status and polluted environment7,16,31.
LIMITATIONS
The present has several has several limitation that warrants consideration. Data were collected in a busy outpatient department setting, which may have posed challenges for participants with limited literacy in accurately comprehending and completing the questionnaires. Additionally, participants may have felt apprehensive while demonstrating intranasal spray technique in a crowded clinical environment, potentially influencing the accuracy of the technique assessment. Furthermore, as this was a single-center study conducted at a national referral hospital, the findings may have limited generalizability to the broader population and to other healthcare settings.
Recommendations
Both awareness and practices among patients receiving intranasal corticosteroid nasal spray were poor. Therefore providing a structured education to patients regarding the correct use, benefits, and safety of intranasal corticosteroids using leaflets, posters, and short instructional videos. Also a further study can be done to assess the awareness and practices among health care providers (ENT technicians, GPs and General duty medical officers) when they treat patients with allergic rhinitis.
CONCLUSIONS
Awareness and practice among patients using intranasal corticosteroid spray for allergic rhinitis are inadequate, likely contributing to poor symptom control. Targeted education and demonstration of proper spray technique may improve adherence and clinical outcomes.
ACKNOWLEDGEMENT
I would like to acknowledge all the ENT technicians for assisting in Data collection. I would also like to thank all the staffs of ENT department for their support during the study
REFERENCES
1. Brożek JL, Bousquet J, Agache I, Agarwal A, Bachert C, Bosnic-Anticevich S, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines—2016 revision. J Allergy Clin Immunol. 2017;140(4):950–8.[DOI] [PubMed]
2. Wise SK, Lin SY, Toskala E, Orlandi RR, Akdis CA, Alt JA, et al. International Consensus Statement on Allergy and Rhinology: Allergic Rhinitis. Int Forum Allergy Rhinol. 2018;8(2):108–352. [DOI] [PubMed]
3. Bousquet J, Schünemann HJ, Togias A, et al. Next-generation Allergic Rhinitis and Its Impact on Asthma (ARIA) guidelines for allergic rhinitis based on Grading of Recommendations Assessment, Development and Evaluation (GRADE) and real-world evidence. J Allergy Clin Immunol. 2020;145(1):70-80.e3. [DOI][PubMed]
4. Naclerio R, Ansotegui IJ, Bousquet J, Canonica GW, D’Amato G, Rosario N, et al. International expert consensus on the management of allergic rhinitis (AR) aggravated by air pollutants: Impact of air pollution on patients with AR: Current knowledge and future strategies. World Allergy Organ J [Internet]. 2020;13(3):100106. Available from: https://doi.org/10.1016/j.waojou.2020.100106 [DOI] [PubMed]
5. Chong SN, Chew FT. Epidemiology of allergic rhinitis and associated risk factors in Asia. World Allergy Organ J. 2018;11(1). [DOI] [PubMed]
6. Klimek L, Bachert C, Pfaar O, Becker S, Bieber T, Brehler R, et al. ARIA guideline 2019: treatment of allergic rhinitis in the German health system. Allergol Sel. 2019;3(01):22–50. [DOI] [PubMed]
7. Ridolo E, Incorvaia C, Pucciarini F, Makri E, Paoletti G, Canonica GW. Current treatment strategies for seasonal allergic rhinitis: where are we heading? Clin Mol Allergy [Internet]. 2022;20(1):1–8. Available from: https://doi.org/10.1186/s12948-022-00176-x[DOI] [PubMed]
8. Yáñez A, Rodrigo GJ. Intranasal corticosteroids versus topical H1 receptor antagonists for the treatment of allergic rhinitis: A systematic review with meta-analysis. Ann Allergy, Asthma Immunol. 2002;89(5):479–84. [DOI] [PubMed]
9. Fokkens WJ, Lund VJ, Hopkins C, Hellings PW, Kern R, Reitsma S, et al. Epos 2020. Off J Eur Int Rhinol Soc Confed Eur ORL-HNS. 2020;Suppl 29:1–464. [DOI] [PubMed]
10.Gani F, Pozzi E, Crivellaro MA, Senna G, Landi M, Lombardi C, et al. The role of patient training in the management of seasonal rhinitis and asthma: Clinical implications. Allergy Eur J Allergy Clin Immunol. 2001;56(1):65–8. [DOI] [PubMed]
11.Sharma RSR. A Study to Assess Knowledge Regarding Prevention of Allergic Rhinitis among Adult Patients Attending General OPD in Selected Hospitals. Int J Sci Res [Internet]. 2017;6(4):74–6.[FULL TEXT]
12.Demoly P, Bossé I, Maigret P. Perception and control of allergic rhinitis in primary care. npj Prim Care Respir Med [Internet]. 2020;30(1):1–6. [DOI] [PubMed]
13.Abdullah B, Kandiah R, Hassan NFHN, Ismail AF, Mohammad ZW, Wang DY. Assessment of perception, attitude, and practice of primary care practitioners towards allergic rhinitis practice guidelines: Development and validation of a new questionnaire. World Allergy Organ J [Internet]. 2020;13(12):100482. [DOI] [PubMed]
14.Albouq NG, Julaidan RA. Prevalence, knowledge, and practice regarding allergic rhinitis among Madinah Population, Saudi Arabia, in 2019–2020. Saudi J Otorhinolaryngol Head Neck Surg [Internet]. 2022;24(2):67. [DOI] [FULL TEXT]
15.Bhargave C, Verma M, Jakes RW, Okamoto Y. Knowledge and Attitude Among Patients and Physicians on Allergic Rhinitis (KAPPA): An International Survey. J Asthma Allergy. 2022;Volume 15(November):1645–64. [DOI] [PubMed]
16.Georgy V, Fahim HI, El Gaafary M, Walters S. Prevalence and socioeconomic associations of asthma and allergic rhinitis in northern Africa. Eur Respir J. 2006;28(4):756–62.[DOI] [FULL TEXT]
17.Navarro-Locsin CG, Romualdez JA. Attitudes, practices on allergic rhinitis of three socioeconomic classes of Filipinos in the National Capital Region. Asia Pacific Allergy. 2016 Apr 1;6(2):94-100. [DOI] [PubMed]
18.Corbett M, Garry S, Mc Gloughlin E, Hinchion K, Keogh I. Treating rhinitis with topical nasal sprays: Patient knowledge, use and satisfaction. Ir Med J. 2020;113(8):1–8.[Full Text]
19.Rajasekaran V, Ghosh P. Knowledge, attitude and practice about allergic rhinitis in a rural population, Kancheepuram district, Tamil Nadu. Int J Otorhinolaryngol Head Neck Surg. 2017;4(1):159.[DOI][Full TEXT]
20.Benninger MS, Hadley JA, Osguthorpe JD, Marple BF, Leopold DA, Derebery MJ, et al. Techniques of intranasal steroid use. Otolaryngol - Head Neck Surg. 2004;130(1):5–24.[DOI][PubMed]
21.Retinasekharan S, Shukri N, Ismail AF, Abdullah B. Knowledge, Attitude, and Practice of Intranasal Corticosteroid in Allergic Rhinitis Patients: Development of a new Questionaere. Health care. Healthcare 2022;10 (8)8-12 [DOI][PubMed]
22.Alreshidi FM, Alrashidi AS, Alshammari FNM. Knowledge, Attitude and Practice about Allergic Rhinitis in Saudi Arabia, 2017. Egypt J Hosp Med. 2017;69(4):2199–203.[FULL TEXT]
23.Retinasekharan S. Development and validation of a new knowledge, attitude and practice questionnaire on allergic rhinitis patients towards intranasal corticosteroid usage [Internet]. Open Access Repository of USM Research & Publication. Univerti Sans Malaysia; 2018.[FULL TEXT]
24.Mohammed IA, Shantier SW, Elhag EA, Osman W. Assessment of knowledge, attitude, and practice of community pharmacists towards allergic rhinitis and its management in Khartoum state: A cross-sectional survey. Informatics Med Unlocked [Internet]. 2022;32(May):101020. [DOI][FULL TEXT]
25.FCL H, HS N. Recent advances in allergic rhinitis. F1000Research [Internet]. 2018 Feb 1 [cited 2021 Jul 8];7(3):202–6. [DOI][PubMed]
26.Gregory C, Cifaldi M, Tanner LA. Targeted intervention programs: Creating a customized practice model to improve the treatment of allergic rhinitis in a managed care population. Am J Manag Care. 1999;5(4):485–96.[PubMed] [FULL TEXT]
27.Bridgeman MB. Overcoming barriers to intranasal corticosteroid use in patients with uncontrolled allergic rhinitis. Integr Pharm Res Pract. 2017;Volume 6:109–19.[DOI][PubMed]
28.Köberlein J, Kothe AC, Schaffert C. Determinants of patient compliance in allergic rhinoconjunctivitis. Curr Opin Allergy Clin Immunol. 2011;11(3):192–9. [DOI][PubMed]
29.Adegbiji WA, Olajide GT, Akeem A, Aluko A. Knowledge , Attitudes and Practices of Health Seeking Behaviours of Parents of Children with Allergic Rhinitis in Nigeria. Journal of Allergy & Therapy. 2022;13(1000272):2–6.[FULL TEXT]
30.Katelaris CH, Lee BW, Potter PC, Maspero JF, Cingi C, Lopatin A, et al. Prevalence and diversity of allergic rhinitis in regions of the world beyond Europe and North America. Clin Exp Allergy. 2012;42(2):186–207.[DOI][PubMed]
31.Wang, Y et al. Allergic Rhinitis Control Test questionnaire-driven stepwise strategy to improve allergic rhinitis control: a prospective study. Allergy vol. 71,11 (2016): 1612-1619.[DOI][PubMed]
|
AUTHORS CONTRIBUTION Following authors have made substantial contributions to the manuscript as under: SJ: Conceptualization, manuscript writing, data collection, data analysis SC: Conceptualization, manuscript writing, data analysis DP: Manuscript writing, data analysis SM: Manuscript writing, data collection Authors agree to be accountable for all respects of the work in ensuring that questions related to the accuracy and integrity of any part of the work are appropriately investigated and resolved. |
|
CONFLICT OF INTEREST None
GRANT SUPPORT AND FINANCIAL DISCLOSURE None
|