ORIGINAL ARTICLE
https://doi.org/10.47811/bhj.201
Assessing the prevalence of noise-induced hearing loss and among Buddhist monks and nuns in monastic institutions in Thimphu, Bhutan: a cross-sectional study
Sonam Tobgay1, Sonam Jamtsho2, Tika Ram Adhikari2, Pelden Wangchuk2
1Department of Ear Nose and Throat, Phuentsholing General Hospital, Chukha, Bhutan
2Department of Ear Nose and Throat, Jigme Dorji Wangchuck National Referral Hospital, Thimphu, Bhutan
Corresponding author:
Dr. Sonam Tobgay
ABSTRACT
Introduction: Noise-induced hearing loss remains underestimated. It is common in factories and in the military due to exposure to loud noise. In Buddhist institutions, various ritual instruments are used daily. Monks and nuns are exposed to different levels of noise in varying frequencies with varying durations, thus predisposing them to noise-induced hearing loss. The existing literature reveals no studies done on noise-induced hearing loss among monks and nuns in Buddhist institutions. Therefore, it is vital to study the prevalence of hearing loss in this group so that appropriate interventions can be implemented. Methods: A descriptive cross-sectional study was performed among Buddhist monks and nuns in monastic institutions in Thimphu, Bhutan. Results: This study revealed the prevalence of noise-induced hearing loss among monks and nuns in monastic institutions to be at 12.34% and a statistically significant association was noted between noise-induced hearing loss and duration of stay in monastic institutions (P=0.01). Conclusion: Monks and nuns are at an increased risk of developing noise-induced hearing loss, and the duration of ritual noise exposure was strongly correlated to the prevalence and severity of the exposure, articulating the cruciality of preventive and rehabilitation measures.
Keywords: Bhutan; Monks; Noise-induced hearing loss; Nuns; Pure tone audiometry.
INTRODUCTION
With rapid development, the world is becoming a noisier place to live in, with sound intensities ranging from 30 dB (decibels) from a person whispering to 140 dB from a powerful firecracker1. The World Health Organization (WHO) estimates that by 2050, one in every ten people worldwide will have disabling hearing loss2. The duration of safe listening time decreases as the sound intensity increases3. The Occupational Safety and Health Administration (OSHA) of the United States of America allows 8 hours of exposure to 90 dB but only 2 hours of exposure to 110 dB sound levels. The NIOSH (National institute for Occupational Safety and Health) would recommend limiting the 8 hour exposure to less then 85 dB. At 100 dB, NIOSH recommends less than 15 minutes of exposure per day4. Noise-induced hearing loss (NIHL) affects communication, productivity, safety and is associated with social isolation, depression, increased risk of dementia, cognitive decline, sleep disturbance and adverse cardiovascular outcomes5-7. Despite its widespread repercussions, NIHL remains an under recognized public health concern, particularly in low and middle-income countries where nearly 80% of people with disabling hearing loss reside8.
The prevalence of NIHL varies across different occupational sectors. In India, studies have reported an 89% prevalence of NIHL among bus transport workers and 48% among those in the agriculture sector. In Pakistan, the prevalence of NIHL among aviation workers was 66%. A study in Iran reported a prevalence of 42.4 % among professional musicians9. Meanwhile, a study in Nepal found NIHL prevalence rates of 31% among carpenters and 44% among sawyers10.
Although NIHL is well documented among factory workers11, musicians9 and military personnel12, research in Bhutan remains limited9,11,12. The Ministry of Health estimated that 0.33% of the Bhutanese population had hearing impairment in 2019 but the types of hearing loss were not specified13. Only one occupational study has explored the prevalence of NIHL in Bhutan14. This study however, doesn’t include monks and nuns, who are routinely exposed to varying frequencies of sounds from ritual instruments, making them more prone to develop NIHL than the general population.
Bhutan is a Buddhist country and has a significant population of monks and nuns in Buddhist institutions across the country. As of 2017, there were 7373 monks, 275 nuns and 461 Gomchens registered with the central monastic body of Bhutan15. The absence of evidence in this population has significant bearing, as unrecognized hearing loss can increase the risk of injury, decrease the productivity of the individual and diminish overall well-being16.
This study aims to determine the prevalence of NIHL among monks and nuns in Buddhist monastic institutions in Thimphu.
METHODS
Study design
A cross-sectional descriptive study was conducted amongst the monastic institutions in Thimphu, Bhutan. The study was undertaken over 3 months, spanning August 2020 to October 2020.
Study setting
Amongst the 26 monastic institutions, 11 are lobdras (primary schools) where the monks begin their training and it is where they have daily ritual practices and training as per their curriculum. Eight are drobdeys, centers for meditation; three are shedras, universities for monks where they focus more on higher studies; three are nunneries, and one is the dratshang, which is the main monastic center in Thimphu.
Study participants
Monks and nuns below the age of 50 years, who provided consent to participate in the study were included. The age limit of 50 was set to remove the confounding effect of presbycusis, an age related to sensorineural hearing loss that typically begins after the age of 50 years. Monks and nuns were excluded if they had active outer, middle or inner ear diseases, pre-existing hearing loss prior to joining monastic schools, or a known history of using ototoxic drugs such as anti-tuberculosis medications, chemotherapy agents, chloroquine or hydroxychloroquine. Those with a history of exposure to blast or gunshot noise, or with congenital hearing loss were also excluded from the study.
Sampling method
A stratified cluster sampling method was used where the monastic institutions were first grouped by category (lobdras, shedras, drobdeys, nunneries, dratshang), and then one institution from each category was randomly selected as the study cluster. The randomization was performed on Microsoft Excel using the stratified randomization function. All monks and nuns from the selected clusters (n=413) were potential study participants.
Study variables
Sociodemographic variables, duration of stay in the monastic institution, average sound level of ritual instruments, duration of exposure to ritual instruments, presence, severity and laterality of NIHL were collected for the study. Pure tone audiometry thresholds were also determined.
Study tool
A structured interviewer-administered research questionnaire was used for collecting data.
Procedure of hearing assessment
Diagnosis of NIHL is based on findings of pure tone audiometry (PTA), a non-invasive hearing test used to identify hearing threshold levels of an individual, enabling determination of the degree, type and configuration of hearing loss using an audiometer.
In this study, PTA was conducted using a diagnostic audio traveler AA220 in a quiet room within the selected monastic institution by experienced audiologists. Although a sound proof room is required for performing PTA, it has been shown that a PTA performed in a quiet room gives a reliable result too. Pure-tone air conduction audiometry was performed to determine the hearing thresholds for both ears of all subjects using an audiometer with earmuffs. Those who had sensorineural hearing loss at 3000, 4000, 6000, 8000 Hz in either one of the ears was taken as NIHL and the severity was graded.
Prior to hearing assessment, sound levels produced by each of the instruments were measured using the NIOSH sound level meter application. NIOSH is free sound level meter app which uses a smartphone’s internal microphone or an external calibrated microphone to measure sound level.
Data analysis
The data collected via the paper-based questionnaires including the findings of PTA was securely digitized in EpiData (version 3.1, EpiData Association, Odense, Denmark) software with double data entry to minimize errors. Statistical analysis was conducted using EpiData Analysis (version 2.2.183, EpiData Association, Odense, Denmark). Descriptive statistics were used to summarize the sociodemographic details, PTA findings. Chi square test was used to identify associations between the duration of years in monastic institutions and NIHL with a p-value < 0.05 being considered statistically significant.
Ethical considerations
Ethical clearance was obtained from the Institutional Review Board (Ref.No.INTERIM IRB/PO20/001/451). Approval of the study was also obtained from the Central Monastic Body and the principals of the monastic institutions before conducting the study (དགེ’རབ’༼ ག༽༢༠༢༠/༡༠༣.). For all participants, detailed information on the study process, right to withdrawal and the potential risks and benefits were explained first and an informed written consent was obtained. For participants aged less than 18 years, a verbal assent was obtained.
Participation was voluntary, with the option to withdraw. Even if the monks were excluded from the study, they were provided treatment for other causes of ear, nose and throat pathology. Participants were anonymized by assigning specific code numbers once the information was gathered. Data confidentiality was maintained with all patient related data being stored under lock and key accessible only to the principal investigator.
RESULTS
Demographics
A total of 389 of the 413 monks present at the institutions met the inclusion criteria and participated in the study. Of these, 351 were monks and 38 were nuns. As shown in Table 1, participants’ ages ranged from 7 to 50 years, with the majority (212, 54.40%) in the 21–30 year age group. Nearly half of the participants (51.41%) had been in monastic institutions for more than 10 years, as depicted in Table 1.
Table 1. Demographics characteristics of the monks and nuns in the monastic institutions during the study period (n=389)
|
Characteristics |
n(%) |
|
Age (years) |
|
|
<=10 |
8 (2.06) |
|
11-20 |
96 (24.68) |
|
21-30 |
212 (54.49) |
|
31-40 |
59 (15.17) |
|
41-50 |
14 (3.59) |
|
Monastic institutions |
|
|
Hongtsho |
38 (9.77) |
|
Pangrizampa |
62 (15.94) |
|
Tango |
116 (29.82) |
|
Simtokha |
71 (18.25) |
|
Tashichodzong |
102 (26.22) |
|
Number of years in the monastic institution |
|
|
<=10 |
189 (48.59) |
|
>10 |
200 (51.41) |
Prevalence and characteristics of noise induced hearing loss
The overall prevalence of NIHL among the monks and nuns was 12.34%. Of the 48 with NIHL, 46 were monks and 2 were nuns. In the majority of participants with NIHL (87.5%), both ears were affected followed by the left and the right ear respectively (Table 2).
Table 2. Laterality of ear affected by NIHL in the monks and nuns in the monastic institutions during the study period (n=389)
|
Side of hearing loss |
n (%) |
|
Both ears |
42 (87.5) |
|
Left ear |
4 (8.3) |
|
Right ear |
2 (4.2) |
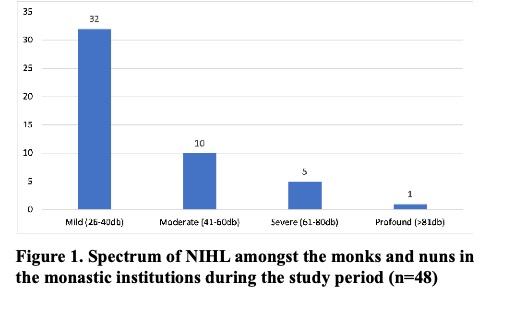
Amongst the monks and nuns with NIHL, the majority (32, 66.7%) had mild degree of hearing loss followed by 20.8% with moderate degree of hearing loss. As reflected in Figure 1, 10.4% had severe degree of hearing loss and 2.0% had profound degree of hearing loss.
Association between prevalence of NIHL and the demographics characteristics
The prevalence of NIHL increased with longer duration of stay in monastic institutions. Among participants who had been in monastic institution for 10 years or less, 7.9% had NIHL. In contrast, among those who had been in monastic institutions for more than 10 years, 16.6% had NIHL. This difference was statistically significant with a p value of 0.014 as shown in Table 3.
Sound produced by instruments used at the monastic institutions
Sound levels produced by instruments used by the monks and nuns were measured using the NIOSH sound level meter application5. As shown in Table 4, Gyaling (trumpet) produced the highest average sound level at 102 dB followed closely by Dung Chen (horn) at 102 dB. The lowest average sound level was produced by drums at 78 dB.
Table 4. Sound level produced by instruments used by the monks and nuns in the monastic institutions during the study period
|
Instruments |
Average sound level (dB) |
|
Gyaling (Trumpet) |
102 dB |
|
Dung Chen (horn) |
100 dB |
|
Cymbals |
96 dB |
|
Bells |
90 dB |
|
Drum |
78 dB |
DISCUSSION
NIHL emerged as a notable occupational health concern among monks and nuns in monastic institutions in Thimphu, with a prevalence rate of 12.34%. Globally, the prevalence of NIHL is estimated to range between 7% and 21% across different regions, as reported by the US NIOSH17. In Bhutan, Pelden et.al reported a prevalence of 27.9% among factory workers14. In comparison, the prevalence of NIHL amongst monks and nuns in this study was 12.34%, which is lower than both the national industrial prevalence and the reported global estimates. However, it is higher than rates reported among administrative industry workers, which was 6.73% in the study by Pelden et al14.The relatively lower prevalence in the monastic population compared to industrial workers may be attributed to the shorter daily exposure durations (approximately 5 hours a day) and the intermittent nature of ritual instrument use with frequent breaks rather than the continuous noise exposure in industries. Additionally, as the study included participants aged 50 years and below, unlike the study done by Pelden et.al who included participants aged above 50 years, this rate does not the represent the true burden of NIHL among the entire monastic population.
Monks are enrolled into monastic institutions as early as four years of age, beginning their education with learning alphabets, spelling and reading, before progressing to memorization of chants and prayers. As they advance in their studies, they specialize in various aspects including the use of ritual instruments18. During the course of their study, they frequently participate in religious ceremonies, during holy months or while performing annual rituals in households. These events represent the periods of greatest noise exposure as instruments are used extensively for the rituals. In this study, the Gyaling (trumpet) was found to produce an average sound level of 102 dB while Dung chen (horn) produced 100 dB, suggesting that monks and nuns are exposed to sound levels comparable to those seen in high-risk occupational settings. For comparison, the average decibel ratings of normal conversation ranges from 60-70 dB, sounds in a movie theaters ranges from 74-104 dB, sounds produced by motorcycles and dirt bikes range from 80-110 dB and sounds produced by sirens range from 110-129 dB19.
A study by Dendup et.al reported that 34.6% of the industries studied in Bhutan had occupational noise levels between 85 and 90 dB, while 38.5% had levels exceeding 91 dB. Carpenters and machine operators were identified as particularly vulnerable to NIHL20. In comparison, this study found that monks and nuns were exposed to cumulative sound levels ranging from 80 to 95 dB during ritual ceremonies, as measured by the NIOSH sound level meter application. This highlights the fact that even religious environments can present noise exposure levels similar to industrial workplaces.
This study found that the majority of monks and nuns with NIHL (66.7%) had mild hearing loss. This pattern is consistent with findings from other studies where individuals with occupational NIHL had a mild degree of hearing loss. For instance, Pelden et al reported that most about 41.6% of industrial workers with NIHL had mild hearing loss, 37.9% had minimal hearing loss, 15.8% had moderate hearing loss, 2.8% had moderately severe hearing loss and 2% had severe hearing loss14. These findings suggest that many affected individuals may remain unaware of their hearing impairment, particularly when symptoms are subtle. This issue is further compounded by the fact that hearing assessments are rarely incorporated into routine health care. According to the Regulation on Occupational Health, Safety and Welfare issued by the Ministry of Labour and Human Resources, employees working in environments where noise levels exceed 85 dBA are required to undergo auditory examination by a qualified medical professional at least once in every six months21. Failure to detect hearing loss early and initiate timely intervention can allow the condition to progress, resulting in greater impact22.This underscores the importance of routine hearing screening and adopting preventive measures to minimize NIHL.
NIHL occurs due to structural or metabolic damage to the cochlea, either from a single intense exposure to an intense “impulse” sound, such as an explosion, or from repeated exposure to loud sounds over time, similar to the exposure monks and nuns experience when playing ritual instruments23. This study demonstrated a statistically significant association between duration of stay in monastic institutions and the prevalence of NIHL (p = 0.010), with those exposed for more than 10 years showing a higher prevalence than those with 10 years or less of stay. Monks and nuns begin training with ritual instruments early in their careers, and the duration of exposure was categorized into two groups (less than 10 years and those more than 10 years) based on evidence from audiometric studies such as one done by Noah et al., which showed that significant NIHL typically appears after a decade of continuous noise exposure24. Similarly, Mohammed et al reported a high prevalence of NIHL among Jordanian industrial workers with over 10 years of noise exposure11. Consistent with this finding, this study observed that NIHL was more prevalent in those with longer duration of monastic life, with 7.9% affected in those with less than 10 and 6.5% in those with more than 10 years of exposure.
Preventive measures such as the use of ear protection during ritual performances and minimizing direct exposure to ritual instruments could substantially reduce the risk of NIHL. In addition, educating monks and nuns on the safe exposure limits and allowable duration of exposure may help prevent its occurrence. This is important as NIHL, once established, is largely irreversible. Interventions can only aim to prevent further auditory damage.
STRENGTH AND LIMITATIONS
This study is the first community-based research conducted to determine the prevalence of NIHL amongst monks and nuns. A limitation of this study is that only four ototoxic medicines were considered for excluding participants, which may not account for all possible confounding factors.
CONCLUSION
This study shows the prevalence of NIHL among monks and nuns in Thimphu to be at 12.34% with a statistically significant association noted between duration of monastic stay and NIHL. These results highlight the cumulative effect of prolonged noise exposure in monastic settings and underscore the importance of routine screening and applying early preventive measures to prevent NIHL. This study also stresses the need for future large-scale studies in monastic institutions around Bhutan so that it will help in mitigating this preventable cause of deafness.
REFERENCES
1. Jacobsen F. Sound intensity and its measurement. In Proceedings of Fifth International Congress on Sound and Vibration. Auburn, AL: The International Institute of Acoustics and Vibration. 1997; 2231-2246. [Full Text]
2. Berglund B, Lindvall T, Schwela DH. New Who Guidelines for Community Noise. Noise Vib Worldw. 2000; 31(4):24–9. [DOI]
3. World Health Organization. Deafness and Hearing loss, 2025. [Accessed on 22nd December 2025] [Full Text]
4. Occupational Safety and Health Administration. Occupational noise exposure. Department of Labor, Occupational Safety and Health Administration, Washington (DC),U.S. 2025. [Full Text]
5. Basner M, Babisch W, Davis A, Brink M, Clark C, Janssen S, et al. Auditory and non-auditory effects of noise on health. Lancet. 2014; 383(9925):1325–32. [PubMed] [Full Text] [DOI]
6. Walling AD, Dickson GM. Hearing loss in older adults. Am Fam Physician. 2012; 85(12):1150–6. [PubMed] [Full Text]
7. Chen Y, Zhang M, Qiu W, Sun X, Wang X, Dong Y, et al. Prevalence and determinants of noise-induced hearing loss among workers in the automotive industry in China: A pilot study. J Occup Health. 2019; 61(5):387–97. [PubMed] [Full Text] [DOI]
8. Bright T, Mactaggart I, Kim M, Yip J, Kuper H, Polack S. Rationale for a Rapid Methodology to Assess the Prevalence of Hearing Loss in Population-Based Surveys. Int J Eniron Res Public Health. 2019; 16(18):3405. [PubMed] [Full Text] [DOI]
9. Pouryaghoub G, Mehrdad R, Pourhosein S. Noise-induced hearing loss among professional musicians. J Occup Health. 2017;59(1):33–7. [PubMed] [Full Text] [DOI]
10.Robinson T, Whittaker J, Acharya A, Singh D, Smith M. Prevalence of noise-induced hearing loss among woodworkers in Nepal: A pilot study. Int J Occup Environ Health. 2015;21(1):14–22. [PubMed] [Full Text] [DOI]
11.Almaayeh M, Al-Musa A, Khader YS. Prevalence of noise induced hearing loss among Jordanian industrial workers and its associated factors. Work. 2018;61(2):267–71. [PubMed] [Full Text] [DOI]
12.Yong JS, Wang DY. Impact of noise on hearing in the military. Mil Med Res. 2015; 2(1):1–6. [PubMed] [Full Text] [DOI]
13.Ministry of Health. Annual Health Bulletin 2020. Health Management Information System and Research Section, Policy and Planning Division, Ministry of Health, Royal Government of Bhutan, 2020;109p. [Full Text]
14.Wangchuk P, Dendup P. Prevalence of occupational noise induced hearing loss in industrial workers in Bhutan. Bhutan Health J. 2020;6(1):25–31. [Full Text] [DOI]
15.Dorji G. Zhung Dratshang: The Central Monk Body of Bhutan. The Druk Journal. 2015. [Full Text]
16.Basner M, Babisch W, Davis A, Brink M, Clark C, Janssen S, et al. Auditory and non-auditory effects of noise on health. Lancet. 2014; 383(9925):1325–32. [PubMed] [Full Text] [DOI]
17.World Health Organization. Addressing the rising prevalence of hearing loss. Geneva: World Health Organization; 2018;9 [Full Text]
18.Dargye Y. An Overview of Bhutan’s Monastic Education System. [Full Text]
19.National Institute on Deafness and Other Communication Disorders. Noise-Induced Hearing Loss. Department of Health and Human Services, National Institutes of Health, Bethesda, US. 2021[Full Text]
20.Dendup P, Tenzin S, Penpa. Epidemiology of Occupational Noise Exposure Level in the Industries of Bhutan. Epidemiol Int. 2019; 4(1):6–9. [Full Text] [DOI]
21.Ministry of Labour and Human Resources Department of Labour. Regulation on Occupational Health, Safety and Welfare, 2022. Ministry of Labour and Human Resources, Department of Labour, Royal Government of Bhutan, 2022. 234p. [Full Text]
22.Kam ACS, Sung JKK, Lee T, Wong TKC, Van Hasselt A. Clinical evaluation of a computerized self-administered hearing test. Int J Audiol. 2012; 51(8):606–10. [PubMed] [Full Text] [DOI]
23.Le Prell CG, Yamashita D, Minami SB, Yamasoba T, Miller JM. Mechanisms of noise-induced hearing loss indicate multiple methods of prevention. Hear Res. 2007; 226(1–2):22–43. [PubMed] [Full Text] [DOI]
24.Seixas NS, Neitzel R, Stover B, Sheppard L, Feeney P, Mills D, et al. 10-Year prospective study of noise exposure and hearing damage among construction workers. Occup Environ Med. 2012; 69(9):643–5 [PubMed] [Full Text] [DOI]